
Focal Renal Lesions
Mindy M. Horrow, MD, FACR, FSRU
July, 2012

Outline
Cysts and cystic conditions
Complex cystic lesions: Bosniakclassification
Primary Malignant Tumors
Primary Benign Lesions
Metastatic disease
Other
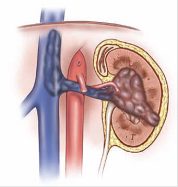
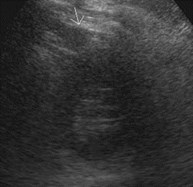
Simple Cyst
CT: water density 10-15 HU,imperceptible wall, no enhancement
US: anechoic, imperceptible wall
MR: signal intensity typical of water,imperceptible wall
“notch”
Bosniak I lesion, a simple cyst
Small simple cyst
Pseudoenhancement of Renal Cysts
Pseudoenhancement (range, 10.3-28.3) may occurwith section collimation equal to or less than 50%of cyst diameter
Effect is maximal with small, 1.5 cm intrarenalcysts which are scanned during maximalparenchymal enhancement
No appreciable enhancement with exophytic cysts
Effect likely related to beam hardening
Maki, etal Radiology 1999;213:468-472
Bae, etal Radiology 2000;216:792-796
Birnbaum, etal Radiology 2002;225:83-90
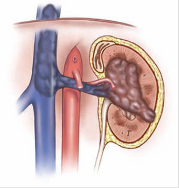
Hereditary Renal Cystic Diseases inAdults: characterized by abnormal ciliaryfunction
Autosomal Dominant Polycystic Kidney Disease
–Abnormal function renal cilium with increased proliferationof tubular epithelium and increased fluid secretion
Medullary Cystic Kidney Disease
Von Hippel-Lindau Disease
Tuberous Sclerosis Complex
Non-Hereditary Renal CysticDiseases in Adults
Acquired cystic kidney disease
–Hyperplasia tubular epithelium with increased risk ofhemorrhage and renal cell carcinoma
Medullary sponge kidney
–Disruption embryonic interface getween ureteral bud andmetanephric blastema
Multicystic dysplastic kidney
–Abnormal differentiation in setting of obstruction duringembryogenesis
Localized renal cystic disease
–Pathogenesis unclear
Katabathina Radiographics 2012;30:1509-1523
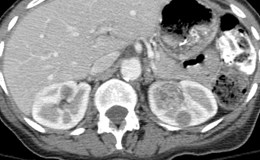
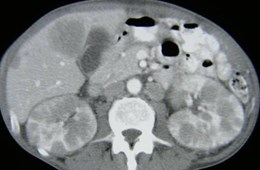
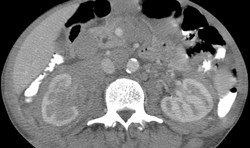
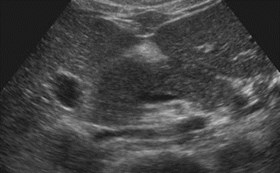
APCKD2 different patients



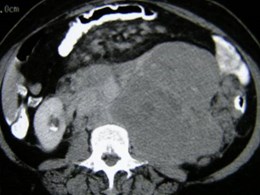
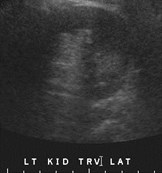
Acquired Cystic Disease of Dialysistwo different patients

Cystic Renal Mass
Calcification
High Attenuation (>20 HU) on unenhanced CT
Signal intensity not typical of water
Septations
Multiple locules
Enhancement
Wall thickening
Nodularity
Bosniak Classification
I – simple benign cyst
II – benign cystic lesions that areminimally complicated
– few, thin septi,
–thin calcifications or short segment of minimallythick, but smooth calcification
–High density, non enhancing lesions < 3cm
Bosniak. Radiology 1986:158;1-10
Bosniak Classification
IIF (follow-up) likely benign but because ofcomplexity require follow up to prove benignity
–More septi
–Minimal thickening
–> 3cm, completely intrarenal high density lesion
–Recommend first follow up at 6 months and thenyearly for 5 years. Cyst can grow, looking forincrease in septations or wall thickening
Israel, Bosniak. AJR 2003:181;627
Bosniak Classification
III- very complex cystic lesion, contrastenhancing thickened septae, usuallyrequire removal but some of these lesionswill be benign
IV- partially cystic but frankly malignant,enhancing components other than wall
Issues with Bosniak Classification
Meticulous, dedicated CT is best modality forcystic mass categorization
Several parameters are qualitative (thickness,calcification)
Greatest inter-observer variability betweencategories II and III
Portion of mass that is most worrisome should beused in deciding category
Issues with applying Bosniakclassification
Small lesion with same type and number ofseptations as large lesion will appear more complex
Enhancement of hyperdense or heavily calcifiedlesions more difficult to assess, especially whensmall
Appreciate concept of pseudo enhancment thatoccurs when relatively small cyst (<2cm) issurrounded by enhancing parenchyma
Freire, Remer. AJR 2009;192:1367-1372
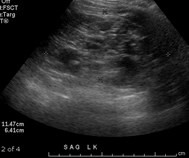
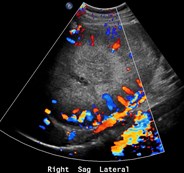
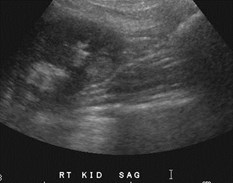
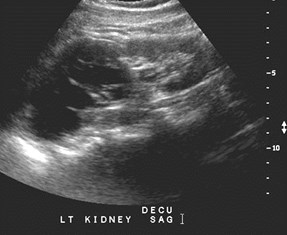
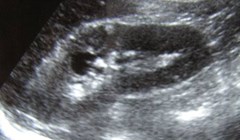
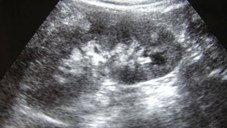
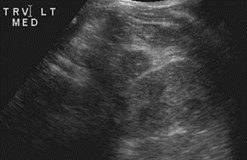
Ultrasound
Many cystic lesions discovered at US
Use highest frequency transducer whichcan penetrate kidney with color andpulsed Doppler for vascularity
Tissue harmonics can reduce noise
Useful in directing biopsies, ablations andpartial nephrectomy
We often find higher Bosniak score on UScompared to CT
CT Technique
Major method for characterizing cystic renallesions
Enhancement: dependent upon dose and rate ofcontrast administration
Triple phase approach probably optimal to look forenhancement and de-enhancement
–< 10 HU = benign cyst
–10 – 20 HU equivocal, but suspicious
–> 20 HU enhancement
MR Imaging
Major role in evaluation renal masses especially inpatients who cannot receive intravenous contrast
T1, T2, enhanced T1
Must standardize signal intensity for each exam.Contrast imaging within single series or imagesubtraction
Bosniak classification can be used, but with somecaveats: superior contrast resolution, inferiorspatial resolution
–Enhancement more obvious
–Septi and wall appear thicker
Bosniak Radiology 2012;262:781-785



Growing simple cyst: Bosniak I

Acute flank pain
Hemorrhage into cyst, no de-enhancement: Bosniak II

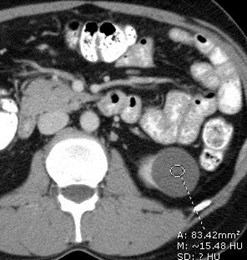
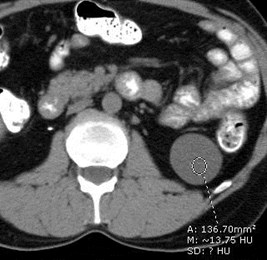
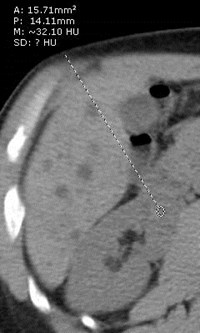
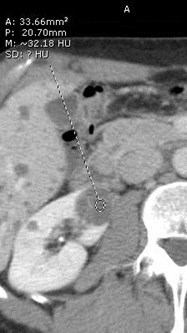
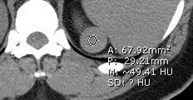
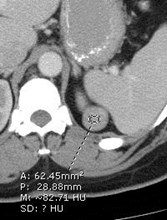
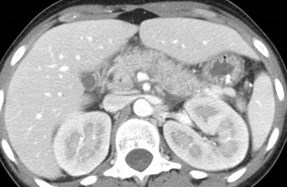
Hyperdense Cysts- Bosniak II Lesion
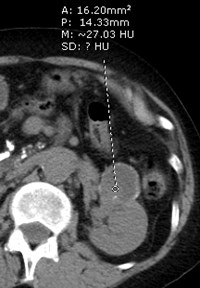
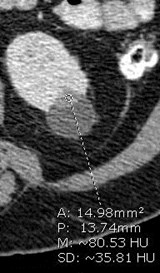
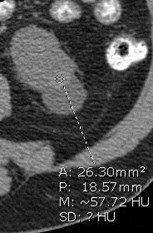
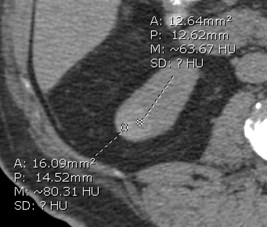
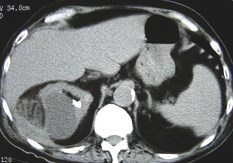
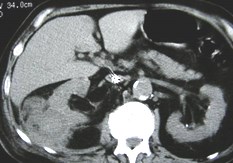
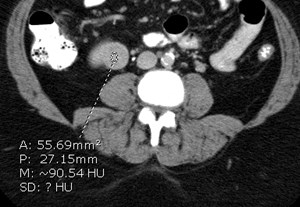
Hyperdense Cyst versus RCC
Non-contrast CT: homogeneous with >70HU, 99.9% hyperdense cyst
Non-constrast CT; hetergeneous with < 60HU likely renal cell carcinoma
Jonisch etal. Radiology 2007; 243:445

Bosniak 2


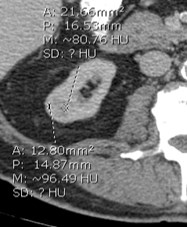
Thin septation, small calcification:Bosniak IIF lesion


Bosniak 2F
Negative for malignancy on aspiration
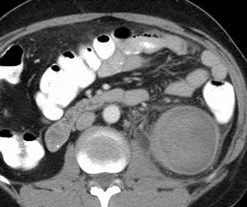
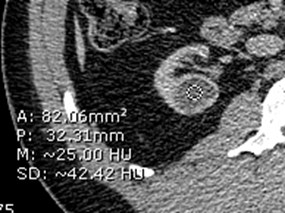
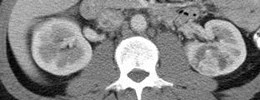
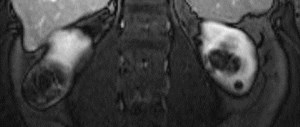
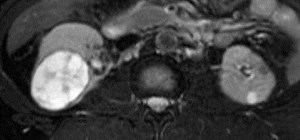
Presumed localized cystic renal disease
Non-Malignant Complex CysticLesions
Localized Cystic Renal Disease-
–uncommon, non-progressive disorder
–characterized by replacement of all or localized areas ofkidney by multiple variably sized cysts
–Aggregate of cysts appear like multiseptate mass, but nodistinct capsule or mural irregularities
Complex Benign Cystic Renal Lesions
–Complex features may be due to hemorrhage, infection,inflammation
–Bosniak II or IIF

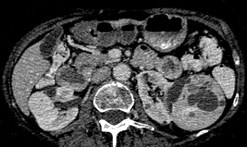
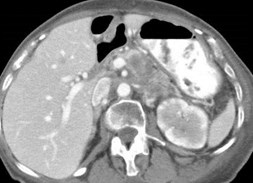
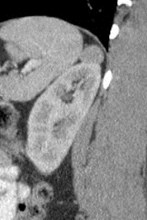
History endstage renal disease
Right simple cysts, left Bosniak III: thick enhancing wall
Papillary renal cancer at surgery

Bosniak 3 Lesion
Multilocular Cystic Nephroma
Outcomes and AssociationsBosniak IIF and III lesions
Retrospective review
–IIF 62 patients
–III 131 patients
Resected lesions
–IIF 4/16 (25%) malignant
–III 58/107 (54%) malignant
Followed lesions
–IIF: 9/69 progressed and 4/8 operated were malignant
Associations
–History of primary renal malignancy, coexisting Bosniak IV lesionsand/or solid mass, multiple Bosniak III lesions were all associatedwith increased malignancy in Bosniak III lesions
Smith, Remer etal. Radiology 2012;262:152
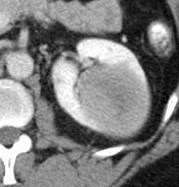
“Bosniak 3”calcified wall limits evaluation



Bosniak 4 with enhancing component


Cystic clear cell carcinoma

Bosniak 4 lesion: measure most suspicious component
Cystic Renal Cell Carcinoma
Papillary type renal cell carcinoma

end stage kidney




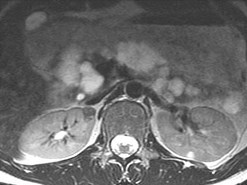
Right Kidney Left Kidney
Bilateral Bosniak 4 lesions: numerousseptations, discreet solid components


Pre C Fat sat
Post C 1 min
Bilateral Bosniak 4 lesions
Bilateral Renal CellCarcinomas
Cystic Tumors
Cystic Clear Cell Carcinoma
–Cystic pattern in 4-15%
–Intrinsic cystic growth, cystic necrosis, origin in epithelium of simplecyst
Multilocular Cystic Renal Cell Carcinoma
–Rare, low grade tumor characterized by multiple septate cystsseparated from kidney by fibrous capsule
–Enhancing septae without any nodules
Multilocular Cystic Nephroma
Mixed Epithelial and Stromal Tumor
–Major female predominance (mean age 52), solid and cysticcomponents
Freire, Remer. AJR 2009;192:1367-1372
Renal Cell Carcinoma
Conventional clear cell -70% Chromophobe- 5%
Papillary (total 15% ) Type 1 Papillary Type 2
Histopathologic Subtypes of RCC
Ng etal. AJR2008;191:1220
Staging
Anatomic extent at diagnosis is single mostimportant factor in prognosis
5 year survival of 60 – 90% with organ confineddisease, 5 – 10% with distant metastases
Cell type also affects survival, spindle andanaplastic tumors with worse prognosis
2 Staging systems: Robson and TNM
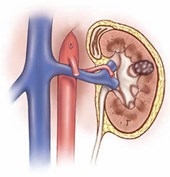
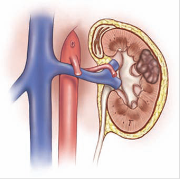
Stage 1 Stage 2 Stage 3A
< 7cm > 7 cm Involving perinephric fat
From Ng. AJR 2008;191:1220
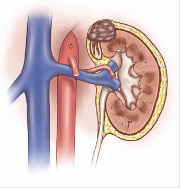
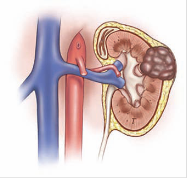
Stage 3A Stage 3B Stage 3C
Adrenal Gland Renal V/IVC SupradiaphragmaticIVC
From Ng. AJR 2008;191:1220
Renal Cell Carcinoma
Regional lymph nodes (N)
NX: Regional lymph nodes cannot be assessed
N0: No regional lymph node metastasis
N1: Metastasis in a single regional lymph node
N2: Metastasis in more than 1 regional lymph node
Laterality does not affect the N classification.
Distant metastasis (M)
MX: Distant metastasis cannot be assessed
M0: No distant metastasis
M1: Distant metastasis
AJCC Staging Groups
Stage I
T1, N0, M0
Stage II
T2, N0, M0
Stage III
T1, N1, M0
T2, N1, M0
T3a, N0, M0
T3a, N1, M0
T3b, N0, M0
T3b, N1, M0
T3c, N0, M0
T3c, N1, M0
Stage IV
T4, N0, M0
T4, N1, M0
Any T, N2, M0
Any T, any N, M1
Renal Cell Carcinoma
Associated genetic conditions: von-Hippel-Lindau,hereditary papillary renal cancer (autosomaldominant), tuberous sclerosis
More common in acquired cystic renal disease,long term dialysis (3-6x risk)
Suggested risk factors: cigarette smoking, obesity,diuretic use, petroleum products, chlorinatedsolvents, cadmium, lead, asbestos, ionizingradiation, high-protein diets, HTN, Renal TX, HIVinfection
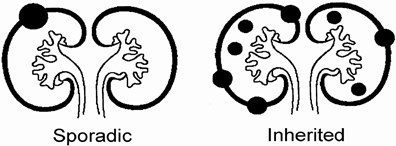
Hereditary Renal Cell Carcinoma
Hallmarks:
–Multiple and bilateral
–Presents at younger age. Sporadic RCC usually in > 60 years
–Equal prevalence in women and men. Sporadic more common in men
–Family history may be positive, variable expressivity
Choyke, etal. Radiology 2003;226:33-46
Hereditary Renal Cell Carcinoma
Types
–Von-Hippel Lindau- RCC clear cell, type cysts,pheochromocytomas….
–Tuberous Sclerosis- AML, cysts, RCC papillary type
–Hereditary papillary renal cancer- papillary type 1
–Hereditary leiomyoma/RCC- papillary type 2 (cutaneous, uterineleiomyomas)
–Birt-Hogg Dube- RCC chromophobe type, also other types
–Hereditary renal oncocytoma
–Medullary carcinoma of kidney- associated with SS trait
–Lynch type 2- RCC clear cell type, associated cancer of colon,endometriaum, ovaries and stomach
Choyke, etal. Radiology 2003;226:33-46
Clear Cell Carcinoma

Without contrast with contrast
Is this a hyperdense cyst?


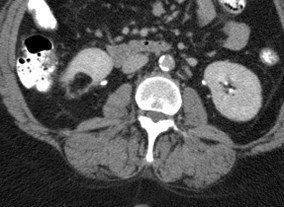
Bilateral Renal CellCarcinomas



Incidental renal cell carcinoma

Hematuria

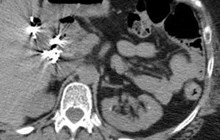
Renal cell carcinomatumor thrombus into IVC
RCC with extension into renal vein,adenopathy, local spread, lung metastases

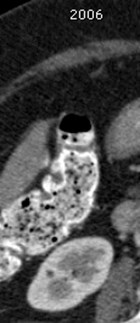
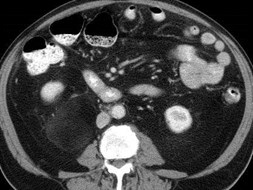
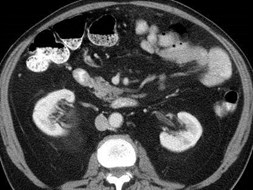
Routine CT for pain
Two years later
Missed renal cell carcinoma: difficulty of cortico-medullary phase


37 year old male with macroscopic hematuria
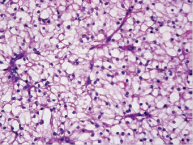
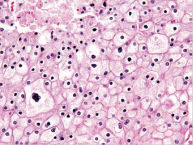
Renal cell carcinoma- chromophobe type
Chromophobe RCC
Third most common type of RCC in < 5%
Hyperechoic on ultrasound
Homogeneous enhancement on CT and MR often withspoke wheel pattern associated with oncocytoma
Similar pathologic features with oncocytoma
> 80% are stage 1 or 2 at presentation
Overall favorable prognosis but may develop hepaticmetastases
Prasad SR Radiographics 2006, 26:1795-1806



Von-Hippel Lindau
Rare autosomal dominant, multi-organ system disease(14) with benign and malignant tumors (40), highpenetrance with variable expression
Most common types and sites of involvement
Death usually 2° RCC or neuro compromise
Screening allows conservative TX to increase length andquality of life
–Hemangioblastomas: retinal, CNS
–Renal cysts (59-63%), tumors (24-45%)
–Pancreatic cysts, tumors
–Pheochromocytomas, endolymphatic sac tumors andepididymal cystadenomas
Leung Radiographics 2008;28:65
Post Operative Surveillance
Radical Nephrectomy
–T1 Yearly CXR
–T2 Abdominal CT @ 2 and 5 years, CXRs
–T3 Abdominal CT @ 2 and 5 years, CXRs
Partial Nephrectomy
–T1- None
–T2 Yearly CXR, Abdominal CT every 2 years
–T3 6-12 mos CXR, Abdominal CT every 6 months for3 years, then yearly
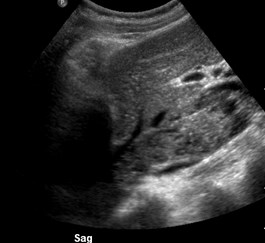
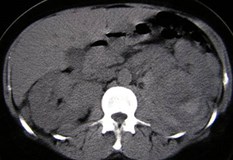
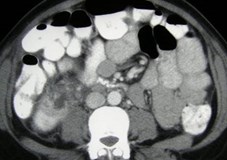
Lymphoma


6 months later



Elevated creatinine


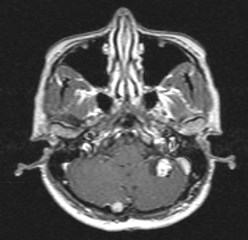
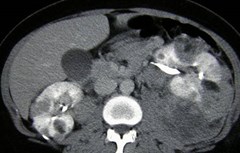
Multifocal lymphoma


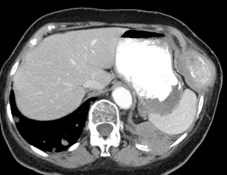
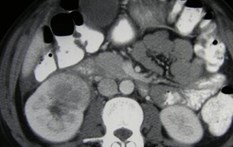
Patient with HIV


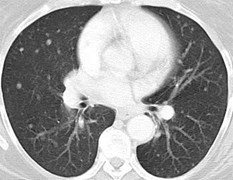
Lymphoma: lungs, liver, kidneys
Imaging Findings in Renal Lymphoma
Multiple masses- typically homogenous, slightlyhyperdense on unenhanced and hypodense afterenhancement
Solitary mass- very rare
Direct invasion from retroperitoneal disease- into renalhila, sinus, parenchyma. May invade and spreadalong ureter.
Diffuse infiltration of kidney without retroperitonealdisease, preserving reniform shape
Perirenal infiltration
Very hypoechoic but without posterior enhancement

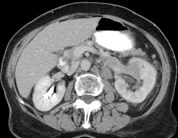
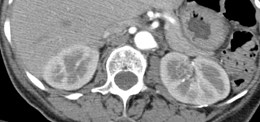
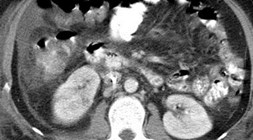
Lymphoma in retroperitoneumgrowing into sinus of kidneys

Diffuse infiltrationboth kidneys
Other manifestations of renal lymphoma

Peri-renal disease
Historical Imaging of Lymphoma






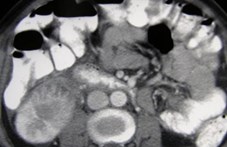
Metastatic thyroid cancer to lung and kidneys

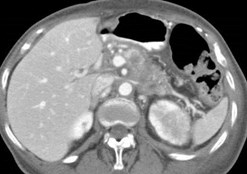
Pancreatic carcinoma metastatic to left kidney



History of lung cancer
Perirenal and adrenal metastases
6 months later
Renal Metastases
Most common primary tumors are lung, breast, GI
Frequency of metastases to kidneys at autopsy is 7% -13%
When renal metastases occur, disease is usually quiteadvanced
Metastases may be expansile or infiltrative
Most frequent pattern is multiple discrete bilaterallesions. Solitary lesions more common with coloncancer and perineprhic tumor extension is typical ofmelanoma.
Difficult to distinguish a single expansile mass from arenal cell carcinoma. Infiltrative lesions tend to bemetastatic


50 yo female
Tubular Spindle Cell Tumor (low grade collecting duct CA)
Described on pathology as large subcapsular mass, predominantlyencapsulated with small focus of invasion into renal parenchyma
Female predominance, favorable outcome



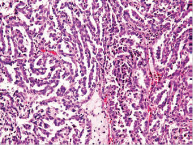
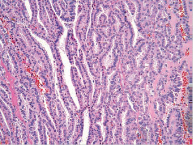
Transitional cell carcinoma
Left flank pain


Blunt trauma patient withhematuria



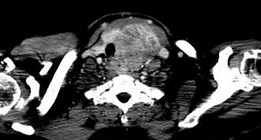
Transitional cell carcinoma

Transitional cell carcinoma with bone metastases
Urothelial tumor of renal pelvis
Predominantly papillary type
Accounts for over 90% renal pelvis tumors, small% are squamous cell
If bladder cancer, 2-4% develop upper tracttumors. If upper tract carcinoma, 20 – 48% risk ofbladder cancer in next 5 years
Bilateral in 2 – 10%
Peak incidence in 60 – 70 years
Biggest risk factor is cigarette smoking


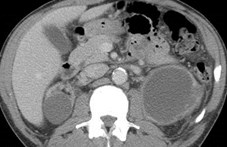
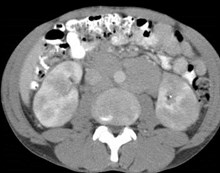
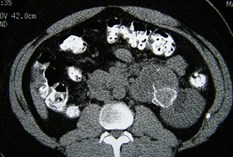
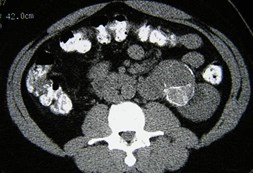
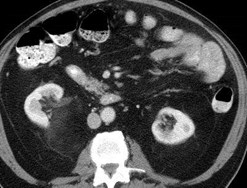
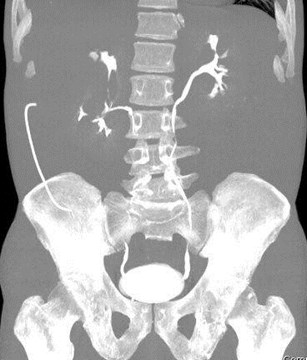
Stone search, left flank pain
Spontaneous hemorrhage from angiomyolipoma
Multiple bilateralangiomyolipomas

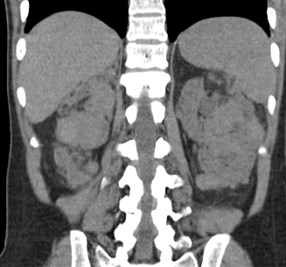

Tuberous Sclerosis
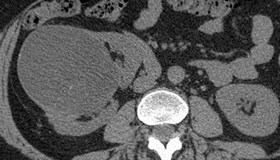
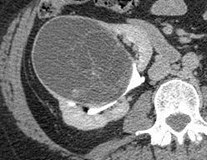
24 year old


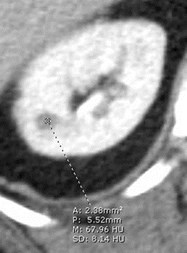
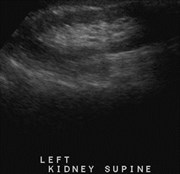
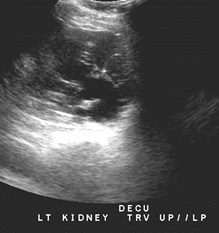
Slowly growing angiomyolipoma

Fat containing lesions on ultrasound measurelarger due to difference in speed of sound
Angiomyolipoma
Benign hamartomas composed of angioid, lipoidand myoid components: intratumoral fat is key toimaging diagnosis
Some contain large angioid component and arehypervascular with small aneurysms whichpredispose to hemorrhage
If < 4cm rarely symptomatic
If > 4cm may require embolization or surgery
Most common benign mesenchymal renal tumor
Small percentage without measureable fat on CT
Angiomyolipoma
Neoplasms of the perivascular epithelioid cells,which are also referred to as PEComas
–Classic triphasic tumors contain visible fat, > 90%
–Monotypic epithelioid are only soft tissue density andthus indistinguishable from RCC (rare, potentialmalignant)
Sporadic AMLs have 4 : 1 female predominance,accounting for 80% of all patients with AMLs
Tuberous sclerosis: 80% have AMLs, accounting for20% of patients with AMLs
Prasad et al. AJR. 2008; 190 (1): 158

Angiomyolipoma
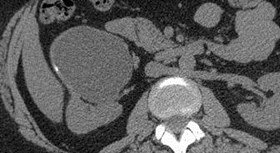
Arise from subcapsular cortex with predominantexophytic growth
Difficult to distinguish from perinephric fat
Look for parenchymal notch to indicate origin oflesion
Liposarcomas are often at periphery of kidney andare exophytic, but typically have no identifiable fat
Liposarcomas (very rare) can arise from renalcapsule or within perinephric space


Renal Lipoma- presumed



Oncocytoma


Oncocytoma



Bilateral Oncocytomas
Oncocytomas
Benign tumors, no metastatic potential
Most common in middle to older agedmen
Homogeneous enhancement on CT
Pseudocapsule, central scar in biggerlesions
“Spoke wheel” arteriographic pattern
Prasad et al. AJR. 2008; 190 (1): 158
Oncocytomas
Typical solitary
May be bilateral in syndromes: multipleoncocytomas, Birt-Hogg-Dubé
Originates from or differentiates towardscollecting duct cells
May be associated with renal cellcarcinoma either as hybrids or collisiontumors
Prasad et al. AJR. 2008; 190 (1): 158





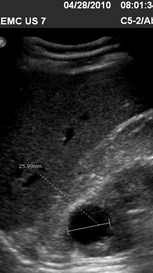
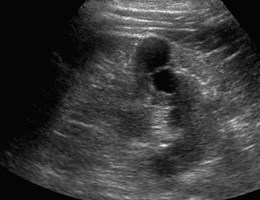
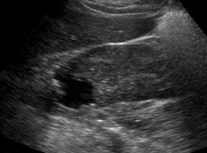
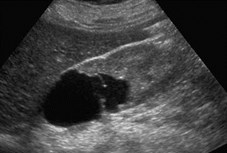
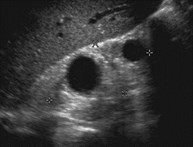
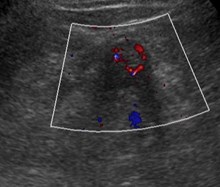
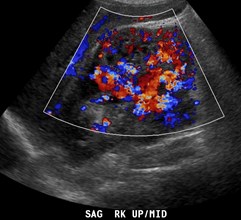
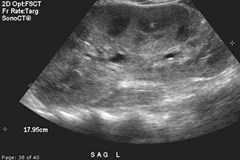
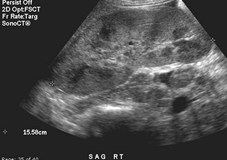
Multilocular CysticNephroma (presumed)



Ultrasound for right upper quadrantpain in a 43 year old woman


Multilocular Cystic Nephroma
Multilocular Cystic Nephroma
50% in males < 3 years
50% in females over 40
Expansile, multiloculated cystic mass
Herniation into collecting system is common
Enhancing septa on CT
Hypo or avascular on arteriography
Differential dx: cystic renal cell carcinoma,segmental multicystic dysplastic kidney, renalabscess

Leiomyoma of renal capsule
Leiomyoma
Rare, benign soft tissue neoplasms,occuring as incidental finding in adults
Most common in renal capsule, butoccasionally in cortex or pelvis
Usually well circumscribed, solid,homogeneously enhancing exophyticmass on CT, but can be quite variable
Prasad et al. AJR. 2008; 190 (1): 158
Other Benign Tumors
Lymphangioma
Hemangioma : associated with Sturge-Weber, Klippel Trenaunay, systemicangiomatosis
Papillary Adenoma
Juxtaglomerular Cell Neoplasm:“reninoma” a rare myoendocrine tumor
Prasad et al. AJR. 2008; 190 (1): 158


Renal Abscess
Right flank pain
Partial resolution after 2 weeks of antibiotics
Focal pyelonephritisbecoming an abscess
Renal Abscess
Clinical findings of infection
Hypoechoic with less throughtransmission than a cyst
Thick wall with rim enhancement on CT
Perinephric inflammation
Neovascularity in wall on angiogram

Focal Xanthogranulomatous Pyelonephritis
XGPN
Focal inflammatory mass may mimic malignancy,filled with lipid laden macrophages
Formed by tumefactive material, non-functional,but some enhancement may occur with contrast
History of chronic UTI
Solid or cystic mass, usually with renal calculus
Best treated with nephron sparing surgery

R
L

Sarcoidosis
Primary manifestation is functional, due toaltered calcium metabolism, may result inmedullary nephrocalcinosis and renalcalculi
Interstitial nephritis (striated nephrogram)and glomerulonephritis
Masses due to granulomatous lesions arevery rare
Radiographics 2004;24:87
Pseudotumors
Angiomyolipoma?
Pre-op: RCC
Partial nephrectomy withfat placed in defect


CT 2 weeks earlier, prior to ESWL
Left flank pain
Pseudotumor due toSubcapsular hematoma
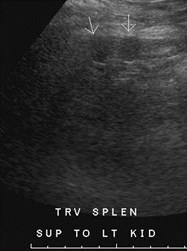
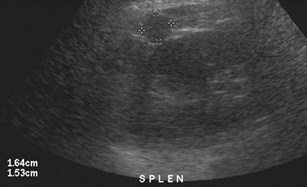
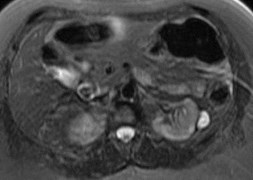
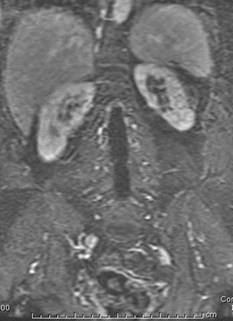
Left Kidney
Pseudotumor dueto splenules


Pseudotumor due to swollentail of pancreas
Suggested Reading
Infiltrative Renal Lesions: Radiologic-Pathologic Correlation Radiographics2000;20:215-243
Current Concepts in the Diagnosis and Management of Renal CellCarcinoma: Role of Multidetector CT and Three-dimensional CTRadiographics 2001;21:S237-S254
A Practical Approach to the Cystic Renal Mass Radiographics2004;24:S101-S115
Renal Cell Carcinoma: Unusual Imaging Manifestations Radiographics2006;26:233-244
Renal Cell Carcinoma: Diagnosis, Staging, and Surveillance AJR2008;191:1220-1232
Imaging Features of Von Hippel-Lindau Radiographics 2008;28:65
Hereditary Renal Cancers Radiology 2003;226:33-46
Can High-Attenuation Renal Cysts Be Differentiated from Renal CellCarcinoma at Unenhanced CT? Radiology;243:445-450